I was recently invited to lead a discussion on assisted dying. I had a few concerns, because I was keen that no one should be upset by the debate, and talking about death and dying will inevitably evoke painful memories, and possibly fear. As I don’t know the histories of the people attending the discussion group, I decided to be very safe, to keep the discussion as impersonal as possible and to encourage discussion at at a very broad, metaphysical level. I personally find details of the ‘mechanics’ of dying perturbing (I don’t think anyone needs to be reminded of what it looks like when food and water are withheld from a patient). I therefore wrote a little talk, to start the discussion and hopefully guide it in a direction that would be helpful, interesting, and not upsetting. This is what I said:

“The debate surrounding assisted dying takes place in a variety of arenas—I have attended debates in government and medical schools and universities. I argue that fundamentally it is also a theological issue—and perhaps it is the philosophers and theologians who should be the loudest voices, though in practice it is the medics and politicians who we mostly hear.
Even the semantics are emotive—are we discussing ‘assisted dying’ or ‘assisted suicide’ or ‘euthanasia’ or ‘mercy-killing’? The terminology can be confusing, so to clarify: ‘Voluntary Euthanasia’—means a doctor will administer medication (Netherlands and Belgium).‘Assisted Dying’—means the medication is provided by a medic, but the patient must take it themselves. (Switzerland, the state of Oregon, and Australia).
I hear people say that it should not be introduced, because ‘Humans are made in the image of God’ (I would love to know what they understand by the image of God) or, ‘Only God should decide life and death’ or ‘Assisted dying is murder, and murder is wrong’.
On the other side of the debate, I hear that ‘We would not allow an animal to suffer, it is cruel to make a human suffer’, ‘Palliative care cannot remove all suffering in all circumstances so we need another choice,’ or ‘Humans should be allowed dignity in life and dignity in death’, or ‘At the moment people have to travel alone to a different country so they can die with dignity’. All of these statements are both true and an over-simplification of the issue.
If we look to the Bible, the issue is one of finding an underlying ethic rather than finding clear examples in the biblical texts. Death in the Old Testament is seen as good (from God—we were created as mortal) and the ‘right’ end to life was die a natural death after a long life, and to be ‘gathered to the ancestors.’ Only premature death (by murder, killing or accident) was seen as a bad thing.
The Bible certainly does not condemn suicide in all cases, as Samson killed himself (and a hall full of enemies) when he pulled down the temple in Judges 17. There are only two cases of ‘assisted dying’ in the Bible of which I am aware. One is in Judges 9:54 (when a man has a millstone dropped on his head by a woman and he would rather a man killed him so he asked his servant to kill him before he died). The other is 1 Samuel 31:4, when King Saul asked his armour-bearer to kill him so that he wouldn’t die by the hand of the enemy. Both of these examples have reasons which today seem unacceptable—but I wonder if they are so different from the motivation today that is sometimes given, of not wanting to be a burden, or not wanting to lose one’s dignity. People want to be in control of their own life, and this includes their own death. In Oregon, reason for assisted dying is most often ‘loss of dignity.’
There are examples in New Testament about ‘laying down life’ for others—such as Jesus, and the good shepherd (for his sheep) and John 15:13 (Greater love has no man than this…) St Paul put himself in danger, and said ‘to die is gain’. This shows that death is not ‘to be avoided at all costs’. (p.35)[1]The New Testament teaches we should love others as Jesus loved us—but should there be limits on this? Should someone feel obligated to ask for assisted suicide, because they don’t want to be a burden on their family, or because they want to spare their family the upset of seeing them as their body deteriorates, or (worse) because they don’t want to use their children’s inheritance to pay for palliative care? How much should love for others obliterate our own rights?
I find it more thought-provoking that in the New Testament, there was the a case which one feels is an obvious time to mercifully aid death. When Jesus was on the cross, he was next to two men, who were also dying, in agony. Crucifixion can take many painful hours to die. One assumes that Jesus, who could summon healing from a distance, would also have been able to summon death, to stop the suffering of the men next to him, who were certainly dying, and who were in agony. Yet he did not. We know that Jesus died first, and that the men had to be killed cruelly (by breaking their legs) for the convenience of the soldiers. It provokes the question of why. Why would Jesus not accelerate death? Is it possible that in dying, people learn something?
Badham suggests the reasons people now want assisted dying are because:
1. People are now enabled to live much longer, and well past the point that they actually want to be alive. (He notes that pneumonia used to be called ‘old man’s friend’ but now it is almost always cured.) As statistics indicate that healthy lifespan is not increasing, the editor of Bulletin of Medical Ethics suggest that the NHS is basically simply involved in ‘the prolongation of dying’. (p.9)
2. People demand autonomy over every area of their lives. People who are used to being autonomous do not wish to be dependent. (p.13)
3. When the medical intervention is stopped (including feeding) death can be slow and painful. (p.14) Dying naturally might not be quick and easy.
Badham examines utilitarianism (the greatest good for the greatest number of people) and states that as 80% of people now want euthanasia in the UK, the law should be changed. (p. 47) He dismisses that this same ethic was used by the Nazis to justify euthanising the handicapped and infirm who did not want to die. (p.53)
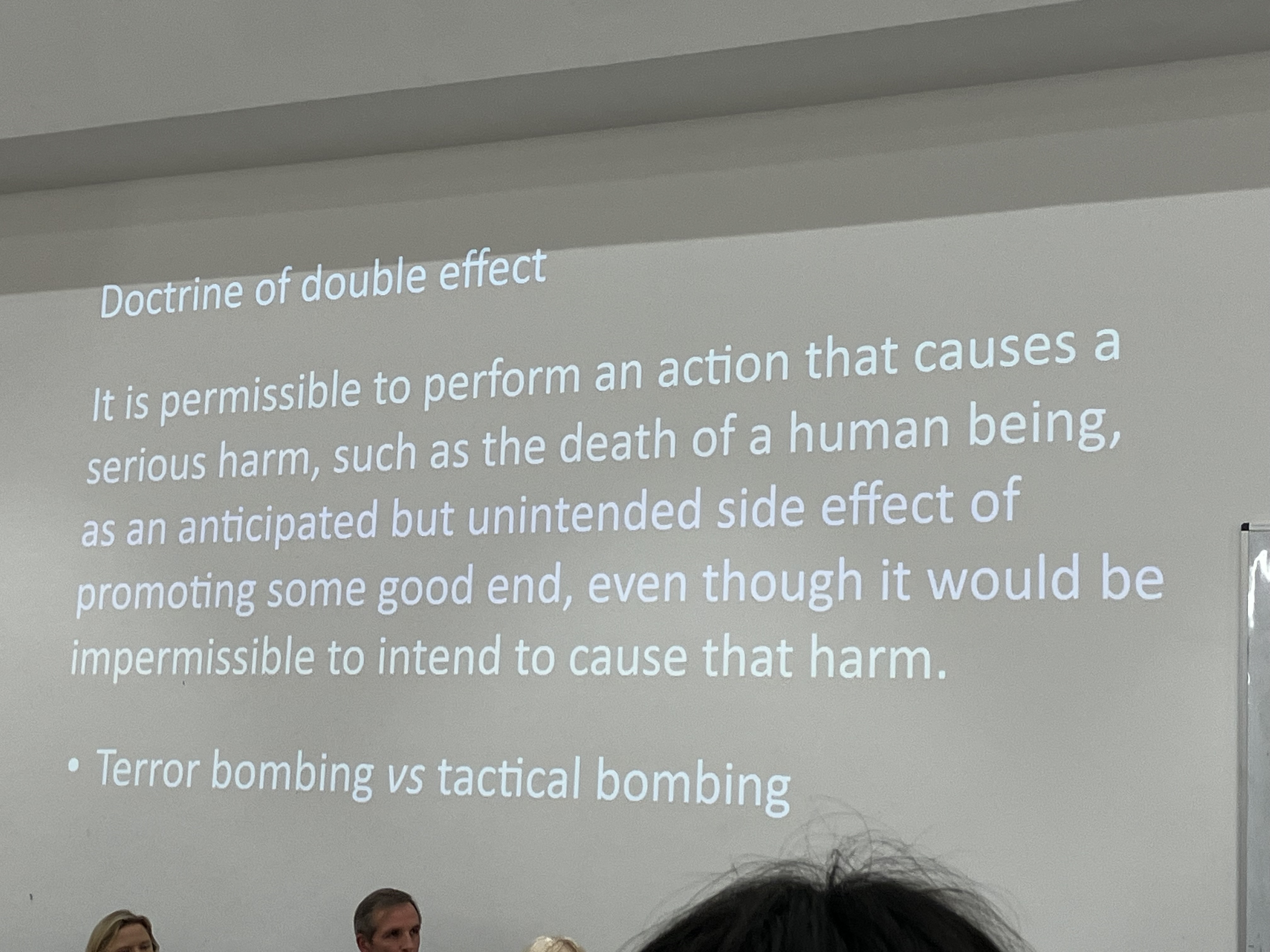
In the UK, doctors can already give life-shortening medication, when death is ‘foreseen but not intended’ and therefore changing the law is simply clarifying what already happens, thus protecting medics from potential law suits. (p.105) At present, the doctor cannot discuss this possibility with the patient, they have to ‘intuit’ that this is what the patient and relatives want, which is open to abuse. Badham says there will be more trust if the situation is more open, and the possibility is legalised formally.
The work of Dr Monika Renz, who undertook research of dying patients in Switzerland, is also relevant.[2] As a psychotherapist and theologian, she helped many patients during the final moments of life, and she suggests that like birth, death is a transition from one state to another. She proposes that understanding this transition enables care-givers and relatives to both help the patient and to view death as a natural process that should not be shortened.
Renz has studied palliative care patients, and concludes that as they die, they pass through a process—which she names ‘transition’—whereby they reach a state where they welcome death and pass peacefully into it. She describes a ‘pre-transition’ phase, when patients often become agitated, they see various ‘visions’ or hallucinations, they feel the need to correct past wrongs or let go of certain relationships. They then reach ‘transition stage, when they relax and are peaceful and all awareness of self/ego appears to have completely disappeared. Like a return to the early stages of life, when a baby is unaware of what it looks like, and bodily functions are of no matter. Renz says this stage can be hard for other people to watch, but for the patient, it is a time of peace. They then gradually slip into death.
This view of death is a natural one. Death is not to be feared, but rather welcomed (and Renz warns against things that force a ‘return to life’ like a last ride in a car, or a visit to a certain place—the patient’s focus should be on letting go, accepting that they are dying.) This tallies with the few references we have of death in the Canon, whereby a character ‘lived to an old age, and then was gathered to their ancestors’.
The implications for assisted dying are therefore somewhat fuzzy. If this process, whilst possibly difficult is also natural, and helpful, and prepares a person for death, then to curtail it would seem wrong. Assisted dying would be akin to sudden unnatural death—which is portrayed as a bad thing in the Canon—like murder or accident. Assisted dying would be to deny a person the time to process what is necessary, to let go of life, to ‘transition’.
‘The inner world of patients and their changing perceptions is strongly related to the spiritual dimension of being, and many dying patients—religious (followers of all religions) as well as agnostic—have impressive spiritual experiences.’ p.6.
‘Nowadays, more and more dying persons proclaim a right to die, as if they owned life and death. The term “self-determination” is misleading: self-determination is important in life to prevent an individual becoming nothing but an object of others, power structures and medical systems. Self-determination however, finds its absolute limits in facing nature, fate, the earth or the divine.’ p.7.
She views humans as essentially spiritual beings (though she avoids using this phrase) and therefore dying is a process whereby a person, whether religious or not, gradually accepts their spiritual identity and moves away from the world with dignity. She writes: ‘such dignity touches on the divine realm, which in post-transition draws close and is almost tangibly present.’ p.43.
She disagrees with the ‘right to die’ or ‘dying with dignity’ campaigns, saying: ‘It is ‘a catchphrase that obscures the question of ultimate human dignity. It is assumed that dignity depends on the autonomous functioning and decision-making capacity of the ego.’ p.117. She goes on to argue that true dignity is found in ‘letting go’ of the ego, and is not something that exists only in relation to how other people view one. She uses children living in poverty as an example, people who have little to ‘offer’ and who suffer daily, yet they still have the right to dignity. She separates ‘dignity’ and ‘autonomy’, saying they are not the same thing and should not be linked. p.117. She views dignity as stemming from God. p.120.
Renz notes there is value in suffering and endurance, and modern society does not value these things and wants to remove them. She worries that health professionals are now pressured to do what people demand, and not what they consider to be right. p.121. (A similar point was made at the Edinburgh debate at the medical school Nov. 2024.)
Badham notes that for Christians, death is not the end—as Bonhoeffer said as he was taken to be hanged: ‘This is the end. For me the beginning of life.’ When Cardinal Hume phoned Timothy Wright, the Abbot of Ampleforth to say he had terminal cancer, the Abbot replied: ‘Congratulations! That’s brilliant news. I wish I was coming with you.’ (p.119)

Questions for Discussion
- When you consider your own experiences of people dying, how much do you think they influence your view on assisted dying? Is this a good basis on which to form an ethical view?
- From a biblical perspective, do you think assisted dying is right or wrong in any circumstances?
- Should a person feel ‘obligated to die’ to spare their relatives inconvenience, embarrassment, sadness, financial loss?
- Should doctors still adhere to the Hippocratic Oath?
- In regard to assisted dying, is it possible to have a rigid ethic that applies to all situations in every age—or does everything depend on circumstances? In what situations do we think killing is definitely right, or definitely wrong?
- Do we think the Bible is still relevant today when deciding contemporary issues?
- The Old Testament presents death/dying as good, ordained by God, a natural planned part of life on earth. What do you consider the good aspects of dying are? What are the bad aspects?
- If we consider the ‘bad aspects,’ which of these will assisted dying address? Could they be resolved differently?
- Do you think that humans should be in control of their own death? If yes, would you place any limits on this, and why? If no, what are your reasons? Are individuals always competent to decide what is an ‘acceptable’ quality of life? If not, who should make that decision? Does dignity depends on the autonomous functioning and decision-making capacity of the ego.’
- Monika Renz states that dying and birth are similar processes, and that in dying we are transformed into a different state. Which of her reasons for a ‘natural death’ do you agree/disagree with?
- If we consider how assisted dying will be implemented, which do you consider to be the biggest problem that must be overcome?
- How should vulnerable people be protected— how will they be protected from coercion?
[1] Paul Badham, Is There a Christian Case for Assisted Dying? (London: SPCK, 2009)
[2] Monika Renz, Dying a Transition trans. Mark Kyburz with John Peck (NY: Columbia University Press, 2015)